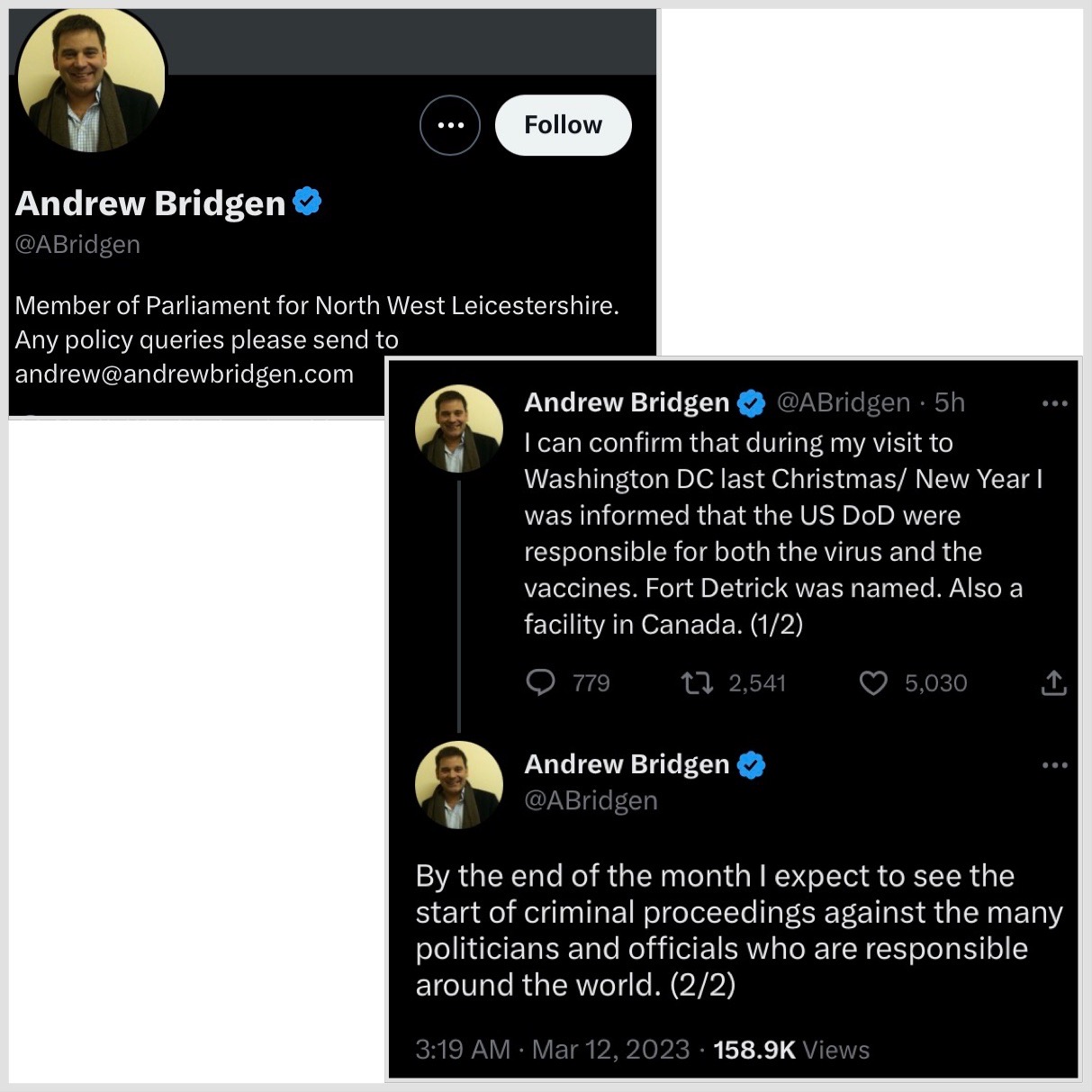
MP Andrew Bridgen says he can confirm he was told the US Department of Defence was responsible for creating COVID-19 and it’s vaccines.
He specifically mentioned Fort Detrick and Canada.
For years, rumours have swirled around Fort Detrick and the bio-lab in Winnipeg. It will be interesting to see if we learn more soon as the MP has suggested. Particularly. now that the world is actually talking about the Wuhan lab and eco health alliance connections to gain-of-function.
Negative effectiveness and deaths. A simplified summary explaining why nobody should take another COVID-19 vaccine.
AlternativeFreePress.com
Part 1 – Negative Effectiveness
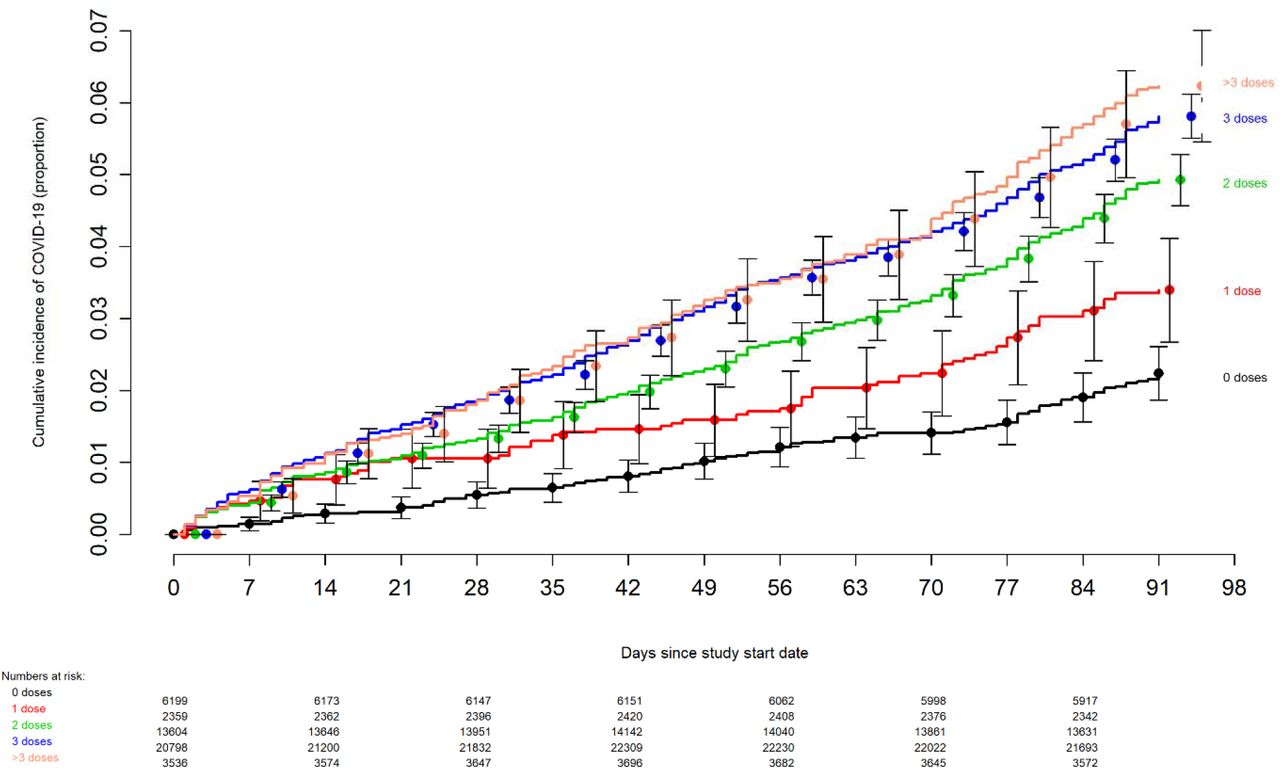
“Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine” studied cumulative incidence of COVID-19 among employees at the Cleveland Clinic following vaccination. The following chart shows that as time passed since vaccination, the incidence of COVID-19 infection increased with each dose. The more doses of vaccine, the higher the proportion of COVID-19 infections.
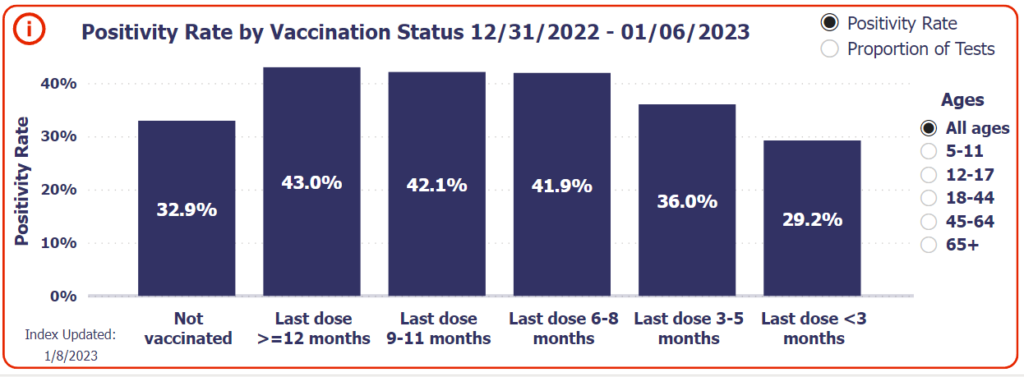
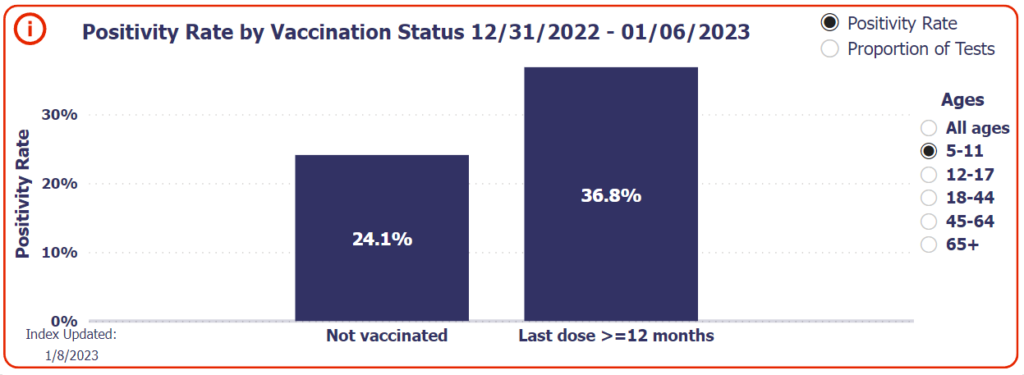
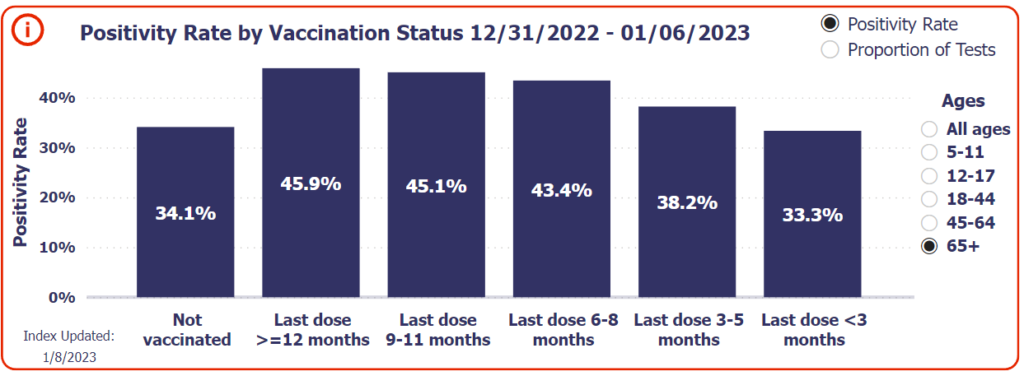
Walgreens has been tracking positivity rate by vaccination status:
Damning enough on its own, but let’s look at how COVID-19 vaccination impacts infections among children exclusively:
Even the elderly are showing negative effectiveness:
This is consistent with what we have been reporting over the past year in Ontario, BC, Scotland, and more.
It is undeniable that the COVID-19 vaccines are not preventing infection, and it seems almost certain that they have increased the infection rate. Let’s look at how….
Part 2 – Antibody Class Switch & Neurodegeneration
Another new paper confirms that mRNA vaccines “induced long-term IgG4 responses – the IgG subclass with inhibitory effector functions. Furthermore, salivary anti-S IgA levels were lower and decreased faster in naïve as compared to pre-infected vaccinees”
Neurological damage is also a problem associated with the COVID-19 vaccines. Researchers have concluded that “neurodegeneration is in part due to intensity and duration of spike protein exposure, patient age, cellular autophagy activity, and activation, function and regulation of p53. Finally, the neurologically damaging effects can be cumulatively spike-protein dependent, whether exposure is by natural infection or, more substantially, by repeated mRNA vaccination.”
Obviously, neurological damage and a broken immune system which produces the wrong antibodies are things most people want to avoid. However, it does help explain why so many people are dying.
Part 3- Vaccinated COVID-19 Deaths
We have been told that the COVID-19 vaccines prevent death. Unfortunately, data from various governments around the world show that, despite Omicron being a less lethal variant, deaths have only increased since the mass vaccination campaign.
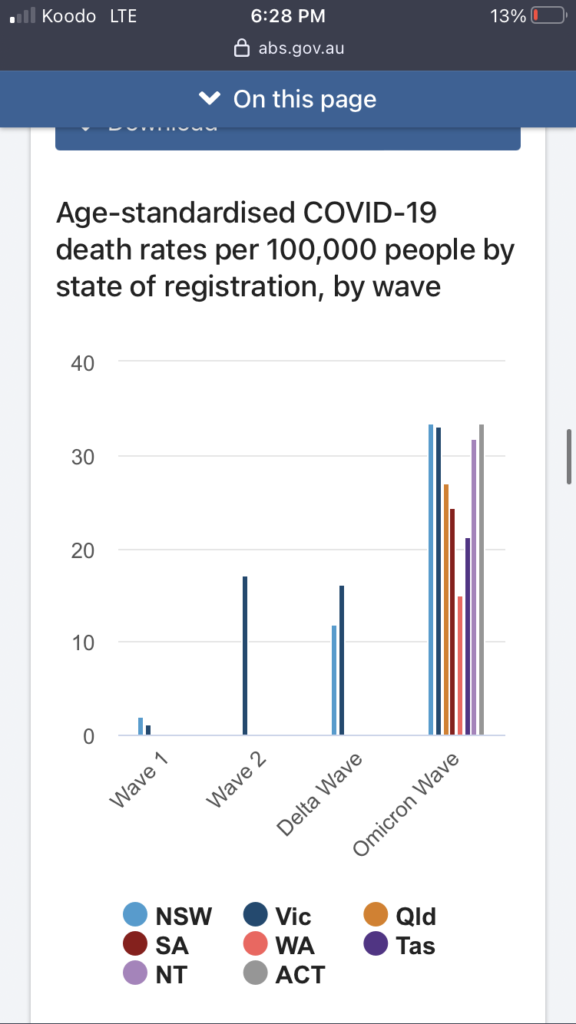
Data from Australia is extremely clear. Almost nobody died from COVID-19 before vaccination. Since vaccination, Australia has seen an explosion of COVID-19 deaths:
In heavily vaccinated Japan, record number of COVID-19 deaths:
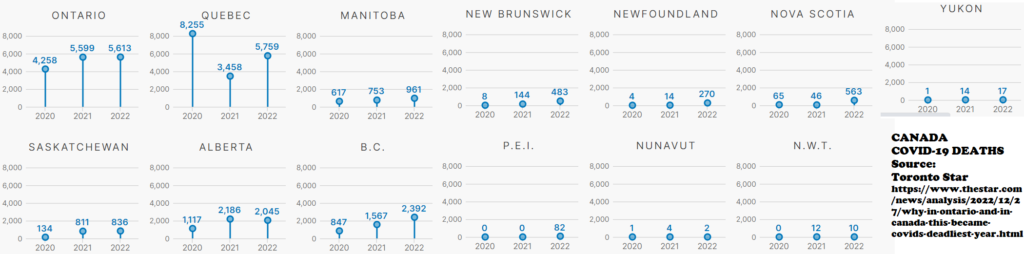
2022 was also the highest number of COVID-19 deaths in Canada:
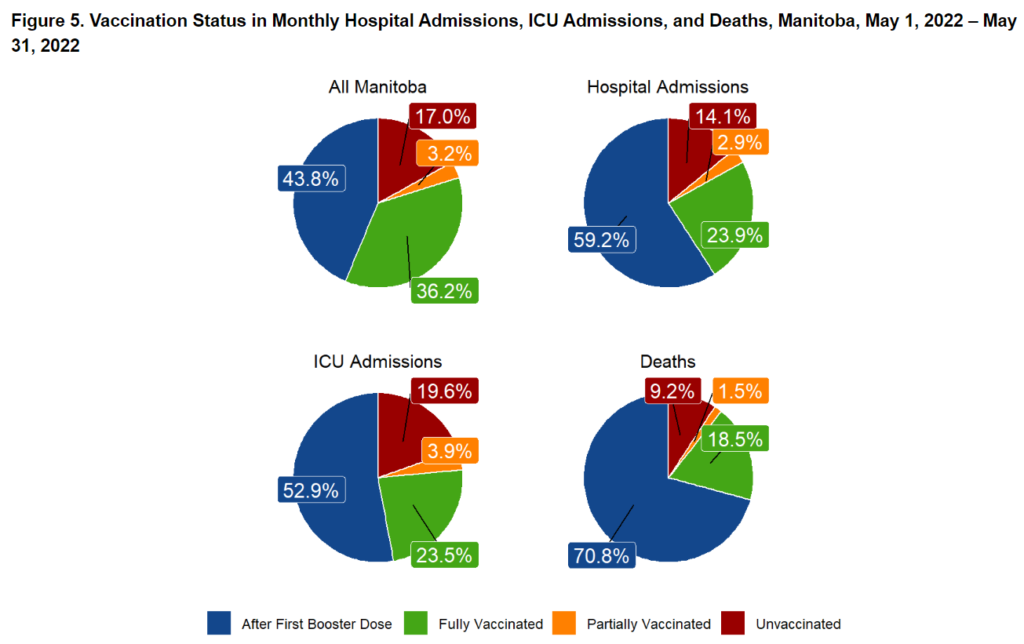
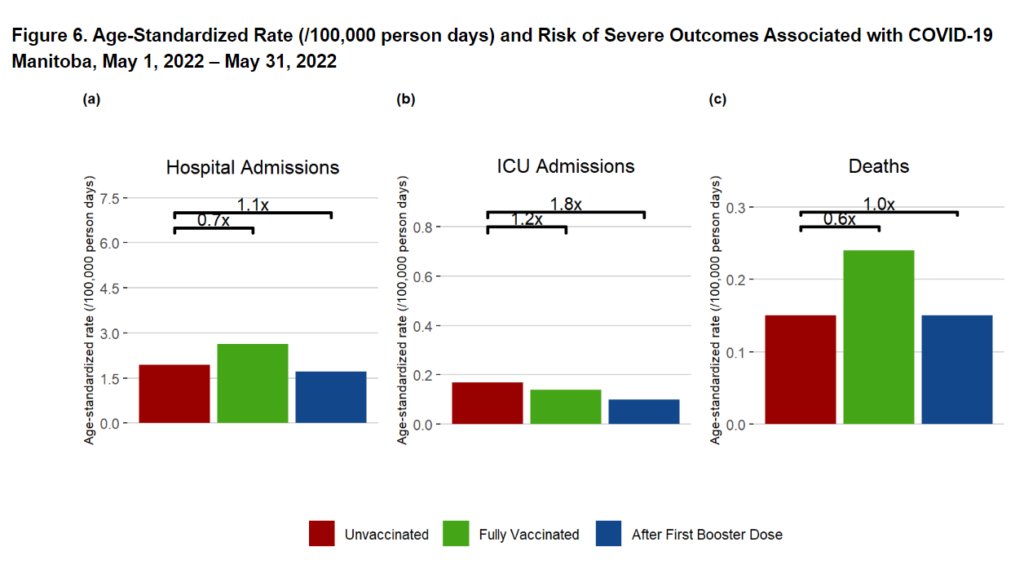
Here is data from Manitoba (2022 week 30 report), it shows a higher rate of death among vaccinated people compared to unvaccinated. The next week they stopped reporting these metrics:
The COVID-19 vaccines are not stopping people from dying of COVID-19. The so called “pandemic of the unvaccinated” has turned out to be quite the opposite with more vaccinated deaths than unvaccinated. Of course, even more people are dying from other causes.
Part 4 – Excess Mortality
In addition to COVID-19 deaths, governments of heavily vaccinated countries around the world have reported excess mortality far exceeding those attributed to COVID-19.
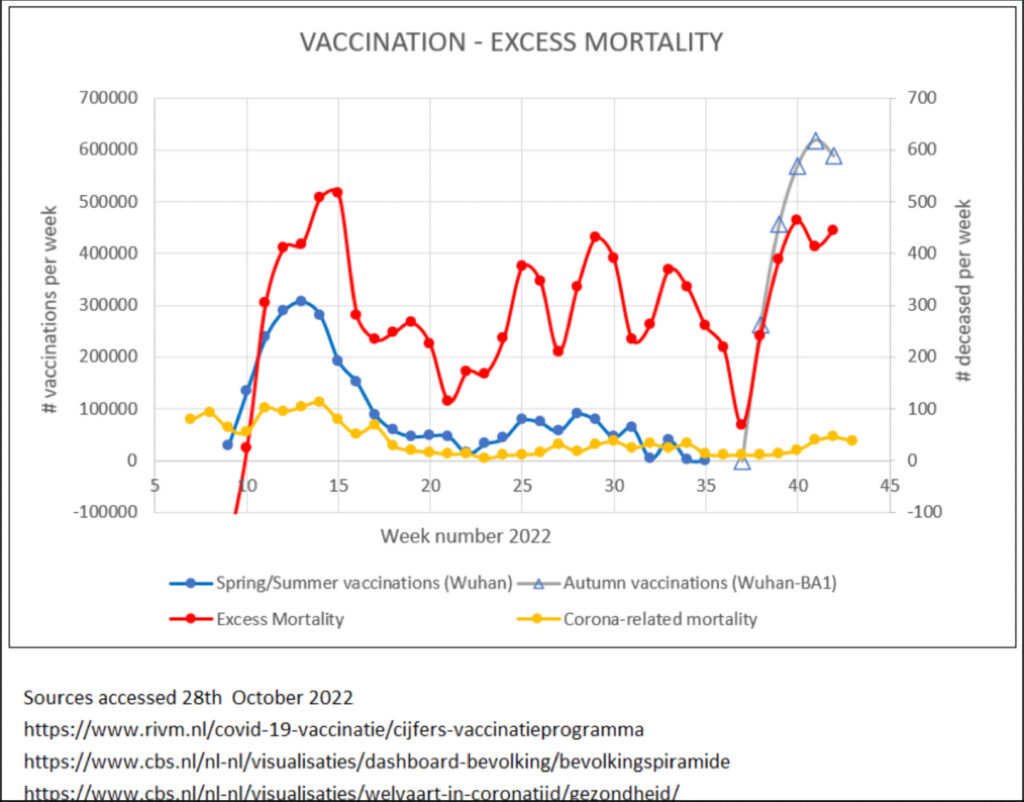
This chart from The Netherlands is especially telling. You can see a huge spike in excess mortality immediately following the start of the vaccination campaign, continued excess mortality throughout 2022, and another spike in excess mortality immediately following the start of the booster campaign.
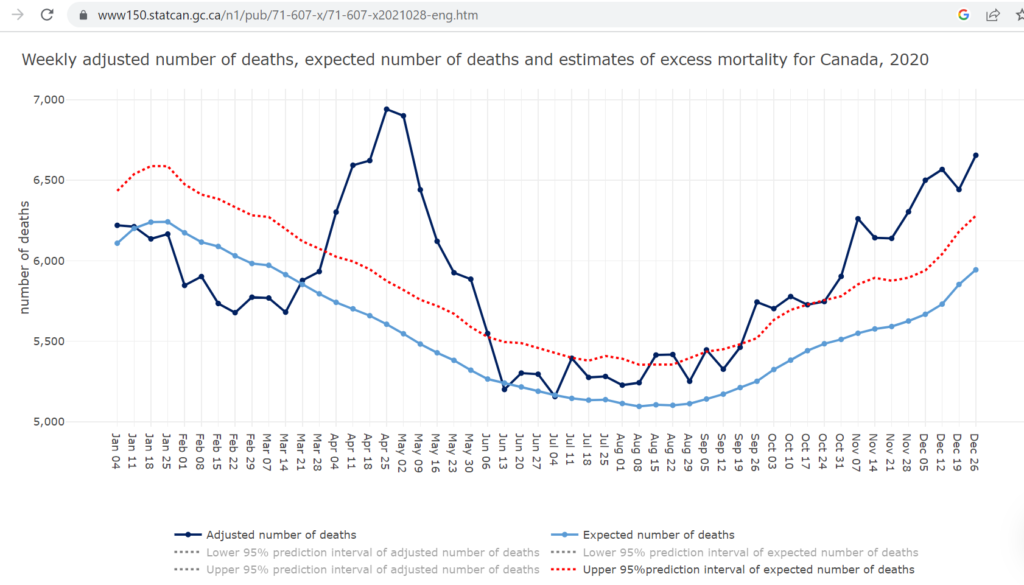
Canada is also experiencing significant excess mortality post-vaccination:
Heavily vaccinated countries around the world are experiencing similar excess mortality to the Netherlands and Canada. What lives are being saved by this vaccination campaign? While we might have extended the lives of some elderly people by a few years, it seems many more young people are falling over dead.
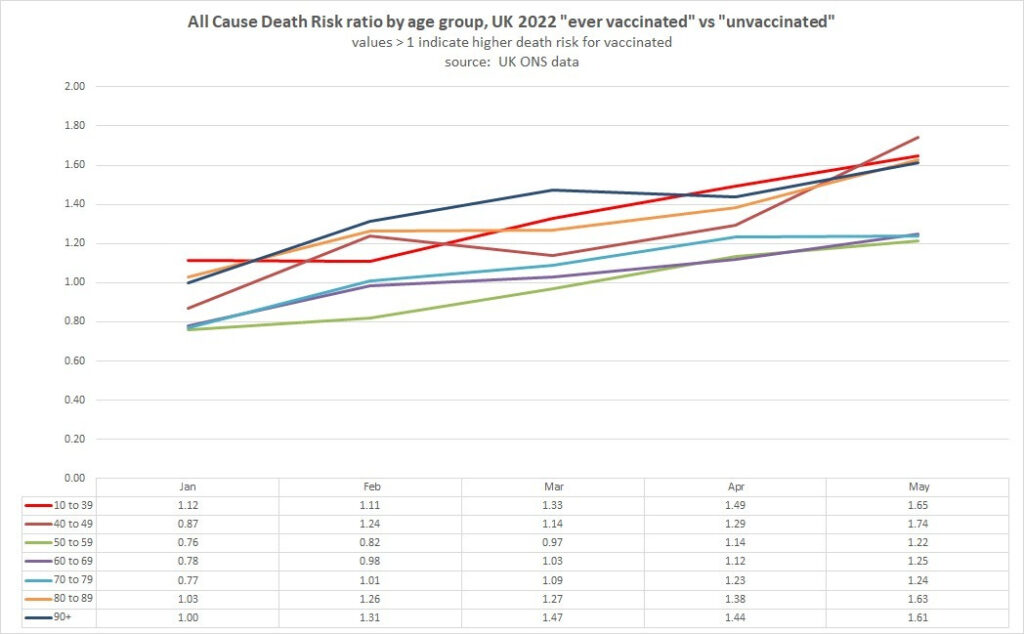
Here is a chart breaking down excess deaths in England. It shows that in the second half of 2022, excess mortality was happening in ALL age categories.
According to the Canadian Journal of Cardiology: Mortality rates from cardiovascular diseases have risen more than those of any other non–COVID-19 ailment. And there are many more people and younger people dying from cardiovascular disease than from COVID-19, at any stage of the COVID-19 pandemic. Similar findings come from the UK. Overall, there has been increasing cardiovascular disease mortality worldwide.
“The mRNA vaccines are not safe, not effective and not necessary,” Conservative MP Andrew Bridgen told Parliament last month. “The Government’s current policy on the mRNA vaccines is on the wrong side of medical ethics, is on the wrong side of scientific data, and ultimately it will be on the wrong side of history.”
Cardiologist Dr. Assem Malhotra warns “the mRNA product is a likely contributory factor in all unexpected cardiac arrests, heart attacks, strokes, cardiac arrhythmia & heart failure since 2021 until proven otherwise’”
Over 17% of teenage vaccine recipients experienced at least one cardiac symptom after the second vaccine dose.
Dr. Peter A McCullough has been warning about the cardiovascular dangers of the COVID-19 vaccines for a year. He has said “The vaccines should be pulled off the market. They clearly are not solving the problem” among many other warnings. He is crystal clear that “they’re not turning out to be safe or effective.”
Could these cardiovascular events be caused by COVID-19 itself? Recent research says NO: Prior to the vaccine launch, the incidence of myocarditis during the pandemic, apparently decreased by 27% compared with a pre-COVID period of time. Additionally, while it has also been suggested that Covid-19 affects the heart through myocarditis, in a study of 37 fatal COVID-19 cases with 21 controls, replication was not detected in COVID-19 hearts using RNA in situhybridization. On top of that, another study found: “There is not yet definitive EMB/autopsy proof that SARS-CoV-2 causes direct cardiomyocyte damage in association with histological myocarditis. Clinical epidemiology data suggest that myocarditis is uncommon for both SARS-CoV-2-positive and -negative PCR cases.” Finally, to put a nail in the coffin of that persistent misconception, COVID-19-Associated cardiac pathology at the postmortem evaluation: a collaborative systematic review found: “The median reported prevalence of extensive, focal active, and multifocal myocarditis were all 0.0%.”
Of course, this leads us to the question of, why are you reading all this on an obscure blog instead of CNN, MSNBC, or even Facebook?
No matter what your opinion about the COVID-19 vaccines, everyone should want transparency and honesty from their media and governments. We now know with absolute certainty that that was not the case with the COVID-19 pandemic.
The FDA has actually been ignoring multiple safety signals. “The fact that the FDA found these four safety signals means they should have followed up on the results and I don’t understand why we haven’t had more information since then. It has been over a year,” says Tracy Høeg, epidemiologist and physician currently conducting covid-19 vaccine research with the Florida Department of Health and California’s Marin County Department of Health and Human Services.
The results of another safety study hidden inside a different study protocol for evaluating boosters by the FDA stated, “In a cohort study of the third dose safety in the Medicare population where historical controls were used, we detected a statistically significant risk for immune thrombocytopenia (incidence rate ratio 1.66, confidence interval 1.17 to 2.29) and acute myocardial infarction (IRR 1.15, CI 1.02 to 1.29) among people with prior covid-19 diagnosis as well as an increased risk of Bell’s palsy (IRR 1.11, CI 1.03 to 1.19) and pulmonary embolism (IRR 1.05, CI 1.0001 to 1.100) in general.”
Whistleblower Brook Jackson documented and reported that an internal audit of the original Pfizer trial was dangerous and violated Federal law. She says that she felt that she had a responsibility to make sure that the participants were protected and that the fraudulent data being collected in the study was not used in any safety and efficacy analysis.
On September 25, 2020, she spoke to an agent at the FDA, and within hours, she was fired by Pfizer.
Recently a leaked video from Israeli Ministry of Health proves with extremely well done research, that the COVID-19 vaccines are unsafe and that serious safety signals have been ignored, that the COVID-19 vaccines cause severe adverse events that do not resolve, and it proves causality.
COVID-19 vaccines are counter-productive at stopping infections. The mRNA vaccines destroy your immune system by causing antibody class switch. They also seem to cause neurological damage, cardiovascular deaths, and rapid cancer progression. Heavily vaccinated countries are experiencing excess mortality, doctors are sounding the alarm, but your government and mainstream media continue to purposefully cover it up.
[JAN 11, 2023 this article has been updated with additional examples of ignored safety signals and fraud]
[JAN 12, 2023 this article was updated with additional evidence that the virus does not cause myocarditis]
[JAN 14, 2023 updated with additional study confirming mRNA vaccines cause class switch and added UK excess death charts]
COVID-19 vaccinations cause depletion of important, virus-fighting IgG3 antibodies and replace them (class switch) with useless IgG4 antibodies. The IgG4 antibodies make the infection seem mild, but fail to clear the virus promptly. IgG4 antibodies have the opposite effect as all other types of antibodies & make our immune system ignore the particular antigen they are trained to detect. Basically, you took an allergy shot to train your body to accept COVID-19 instead of reject it.
IgG3 and IgG4 are subtypes of IgG antibodies, which are the most common type of antibody in the body. Both IgG3 and IgG4 are produced by long-lived plasma cells, which are a type of immune cell that produces antibodies.
IgG3 and IgG4 are structurally similar to each other and to other subtypes of IgG antibodies, but they have some differences in their biological properties.
One main difference between IgG3 and IgG4 is their affinity for certain types of antigens. Affinity refers to the strength of the interaction between an antibody and an antigen. IgG3 has a higher affinity for antigens compared to IgG4, which means that it is more strongly attracted to and binds more tightly to certain antigens. This difference in affinity can affect the ability of IgG3 and IgG4 to neutralize pathogens or stimulate an immune response.
Another difference between IgG3 and IgG4 is their role in the immune response. IgG3 is more effective at activating the complement system, which is a group of proteins that help to kill pathogens and stimulate an immune response. In contrast, IgG4 is less effective at activating the complement system and is more likely to inhibit the immune response.
IgG4 is less effective at binding to and neutralizing certain types of antigens compared to IgG3, which means that it may not be as effective at protecting against certain pathogens. In addition, IgG4 is less effective at activating the complement system, which is a key component of the immune response that helps to kill pathogens and stimulate an immune response. The inability of IgG4 to effectively activate the complement system may further reduce its effectiveness at protecting against certain pathogens.
Given the relative effectiveness of IgG3 compared to IgG4 at neutralizing pathogens and activating the immune response, a vaccine that encourages the production of IgG4 rather than IgG3 would likely be less effective at protecting against certain viruses and other pathogens. It’s also important to consider that the effectiveness of a vaccine is usually evaluated through clinical trials, which involve administering the vaccine to a large group of people and measuring the immune response it elicits and its ability to protect against the targeted pathogen. Skipping clinical trials can increase the risk of a vaccine or medical product, as it may not have been thoroughly tested in a controlled setting and may have unknown risks or side effects.
“Vaccines that induce an antibody response with a stronger skew toward IgG1 and IgG3 may offer better protection, potentially due to superior naturalization capacity. In contrast an immune environment with robust IgG2 and IgG4 response may contribute the disease progression.”several months after the second vaccination, SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG4, which were further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections. IgG4 antibodies among all spike-specific IgG antibodies rose on average from 0.04% shortly after the second vaccination to 19.27% late after the third vaccination. This induction of IgG4 antibodies was not observed after homologous or heterologous SARS-CoV-2 vaccination with adenoviral vectors. Single-cell sequencing and flow cytometry revealed substantial frequencies of IgG4-switched B cells within the spike-binding memory B-cell population (median 14.4%; interquartile range (IQR) 6.7–18.1%) compared to the overall memory B-cell repertoire (median 1.3%; IQR 0.9–2.2%) after three immunizations. Importantly, this class switch was associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition. Since Fc-mediated effector functions are critical for antiviral immunity, these findings may have consequences for the choice and timing of vaccination regimens using mRNA vaccines, including future booster immunizations against SARS-CoV-2.all H4 subtypes were able to neutralize SARS-CoV-2. However, H4-IgG3 exhibited an up to 50-fold superior neutralization potency compared with the other subclasses. Our data point to a strong protective effect of IgG3 Abs in SARS-CoV-2 infection and suggest that superior neutralization might be a consequence of cross-linking the SP on the viral surface.
In summary, the mRNA vaccines encourage the production of IgG4 rather than IgG3, which are not effective at neutralizing pathogens or stimulating an immune response. The body ends up producing far more IgG4 than igG3, which is the opposite of what you would want from a vaccine. IgG3 is 50x better at neutralizing Covid-19. People are not training their immune systems to fight off Covid-19, instead they are training their body to accept disease progression.
I encourage you to view the articles by Rintrah, Jessica Rose, and Igor Chudov listed below as they understand this far more than I do and go into much more depth on the subject.
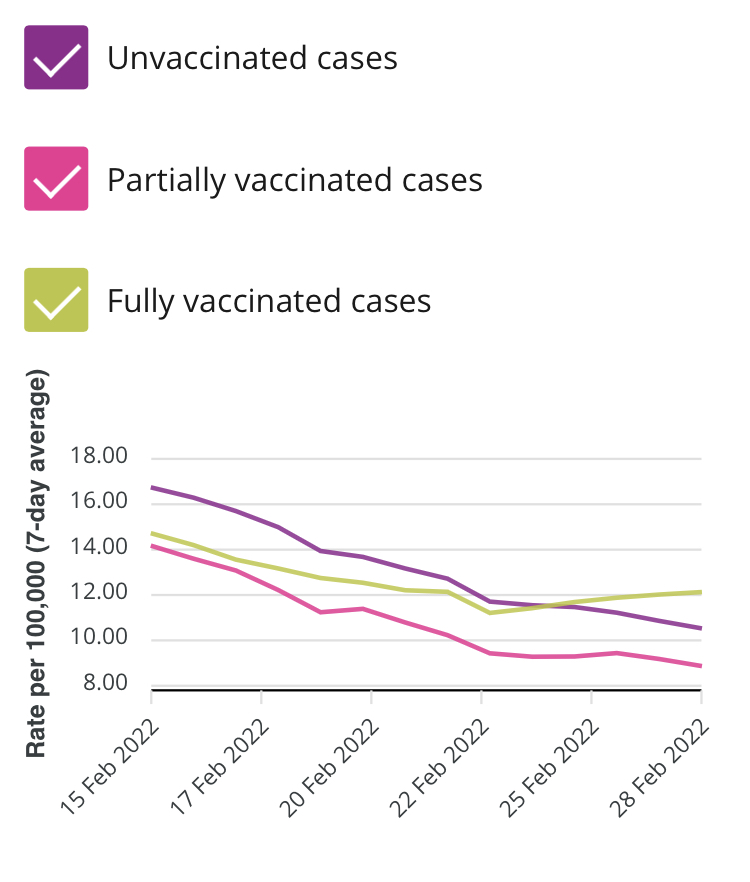
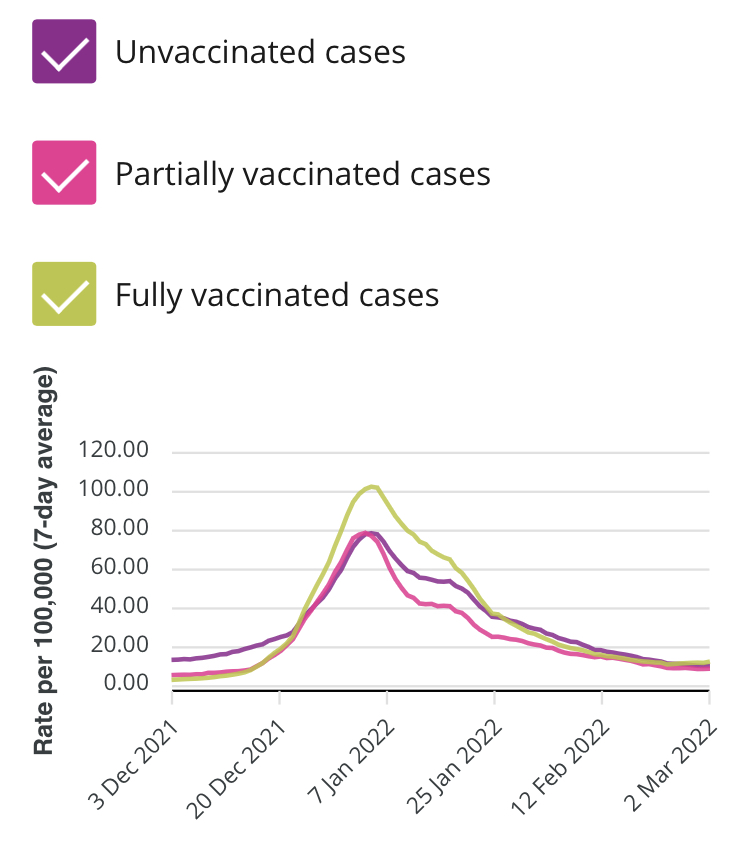
Between late December and late January, vaccinated people in Ontario were infected at a higher rate than vaccinated people . In late January this switched to a higher rate among unvaccinated , however by late February this reversed again. Vaccinated people are now being infected with COVID at a higher rate than unvaccinated people in Ontario for the second time this year.
Haaretz reports “On January 29, ministry figures showed the death rate per 100,000 people under 60 to be 0.1 for the unvaccinated, 0.2 for the partially vaccinated and zero for the fully vaccinated” in Israel.
In Israel “partially vaccinated” includes people who have received 1 or 2 doses.
This means that people under 60 years old who have been vaccinated with 1 or 2 doses are dying at twice the rate of unvaccinated people in Israel.
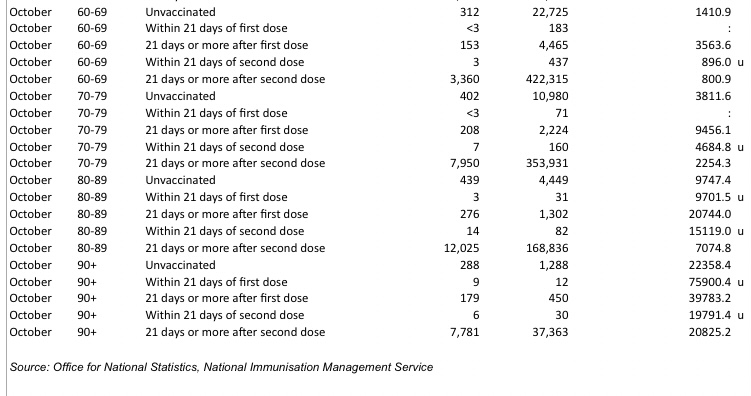
The UK has released data for deaths up to October 2021, and it shows seniors who are vaccinated with one dose are dying at a faster rate than unvaccinated seniors.
Age-standardized mortality rate per 100000 person years :
Age 60-69: unvaccinated mortality 1410.9 >21 days since first dose 3563.6
Age 70-79: unvaccinated mortality 3811.6 >21 days since first dose 9456.1
Age 80-89: unvaccinated mortality 9747.4 >21 days since first dose 20744
Age 90+ unvaccinated mortality 22358.4 >21 days since first dose 39783.2 <21 days since first dose 75900.4
Vaccinated elderly people in British Columbia are being hospitalized at a much higher rate than unvaccinated people. According to this chart from the BCCDC, people over 70 with 2 doses are hospitalized at a rate 80x higher than unvaccinated over 70. (Editor’s note: It seems possible this is an error with ZERO unvaccinated over 70 in hospital, however they have yet to correct it if it is)
The data also shows that boosted individuals make up a whopping 44% of deaths, while only making up 18% of the population. Notably, this is a higher increase than the unvaccinated. While the unvaccinated proportion of death is under double the unvaccinated population, the boosted proportion of death is well over double the boosted population. (Editor’s note: these number have been changing rapidly, this is just a snapshot in time)
Here are 3 charts from Scotland. The first chart shows case infection rate, which shows vaccinated infected at over 2x the rate of unvaccinated.
But where it really gets interesting is deaths and hospitalizations. Scotland is now showing a higher rate of hospitalization and deaths among 2 dose recipients.